 Global Site
Global Site Prevention of Acute Kidney Injury
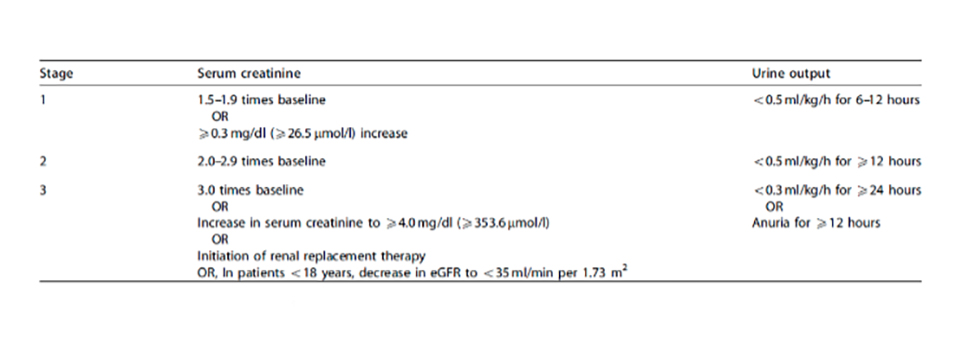
An estimated 50% of ICU patients will suffer from at least one stage of Acute Kidney Injury (AKI) after a length of stay exceeding 24 hours. Studies have shown that mortality is significantly higher for AKI patients (27 % vs. 6%), as is their length of stay (3-10 days vs. 2-6 days) [3] and indicated that patients do not die from comorbidities ‘with AKI’ but die ‘from AKI’ [4]. According to the International Society of Nephrology (KDIGO Guidelines) AKI is staged for severity according to the following criteria:
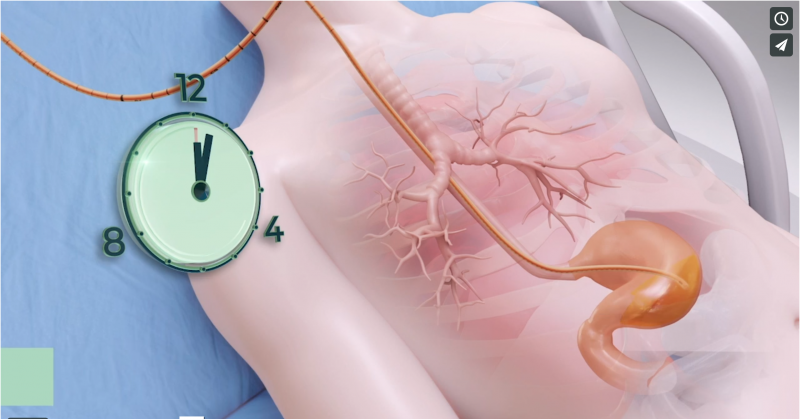
Timely urine output analysis is crucial for the prevention of acute kidney injuries which often result in longer hospital stays and increased mortality rates among ICU patients. Adding urine output criteria to AKI detection methods has been found to detect AKI on average 11h earlier than serum creatinine criteria alone [6]. Ideally, urine output should be checked once per hour, but cumbersome manual observations and documentation are often not carried out frequently enough, due to time constraints faced by health care practitioners. Furthermore, manual observation is often inaccurate.
smART+ reduces the nurses’ burden by automatically and continuously monitoring urine flow.
Abnormalities in flow rate, such as a future increase or decrease in urine output, are predicted in real-time, and alerts based on the KDIGO guidelines are issued to the medical staff before kidney function can deteriorate to a critical level. smART+ assists in detecting all stages of Acute Kidney Injury as early as possible.
[3] Luo X, Jiang L, Du B, et al. A comparison of different diagnostic criteria of acute kidney injury in critically ill patients. Crit Care. 2014;18(4):R144. Published 2014 Jul 8. doi:10.1186/cc13977.
[4] M.E. Thomas, C. Blaine, A. Dawnay, M.A.J. Devonald, S. Ftouh, C. Laing, et al., The definition of acute kidney injury and its use in practice, Kidney International. (2015).https://www.sciencedirect.com/science/article/pii/S0085253815300351 (accessed July 7, 2020).
[5] Khwaja, A. (2012). KDIGO Clinical Practice Guidelines for Acute Kidney Injury. Nephron, 120(4), c179-c184. doi: 10.1159/000339789.
[6] Koeze, J., Keus, F., Dieperink, W., van der Horst, I., Zijlstra, J., & van Meurs, M. (2017). Incidence, timing and outcome of AKI in critically ill patients varies with the definition used and the addition of urine output criteria. BMC Nephrology, 18(1). doi: 10.1186/s12882-017-0487-8.3
Written by
Share